When your eye feels red, painful, and sensitive to light - especially if you're seeing floaters or your vision suddenly blurs - it's easy to brush it off as just tired eyes. But if these symptoms come on fast, they could be signs of uveitis, a serious eye condition that can steal your vision if left untreated. Uveitis isn't just a simple irritation; it's inflammation deep inside the eye, and it's one of the top three causes of blindness worldwide. The good news? If caught early, it's often treatable. The key is knowing what to look for and acting fast.
What Exactly Is Uveitis?
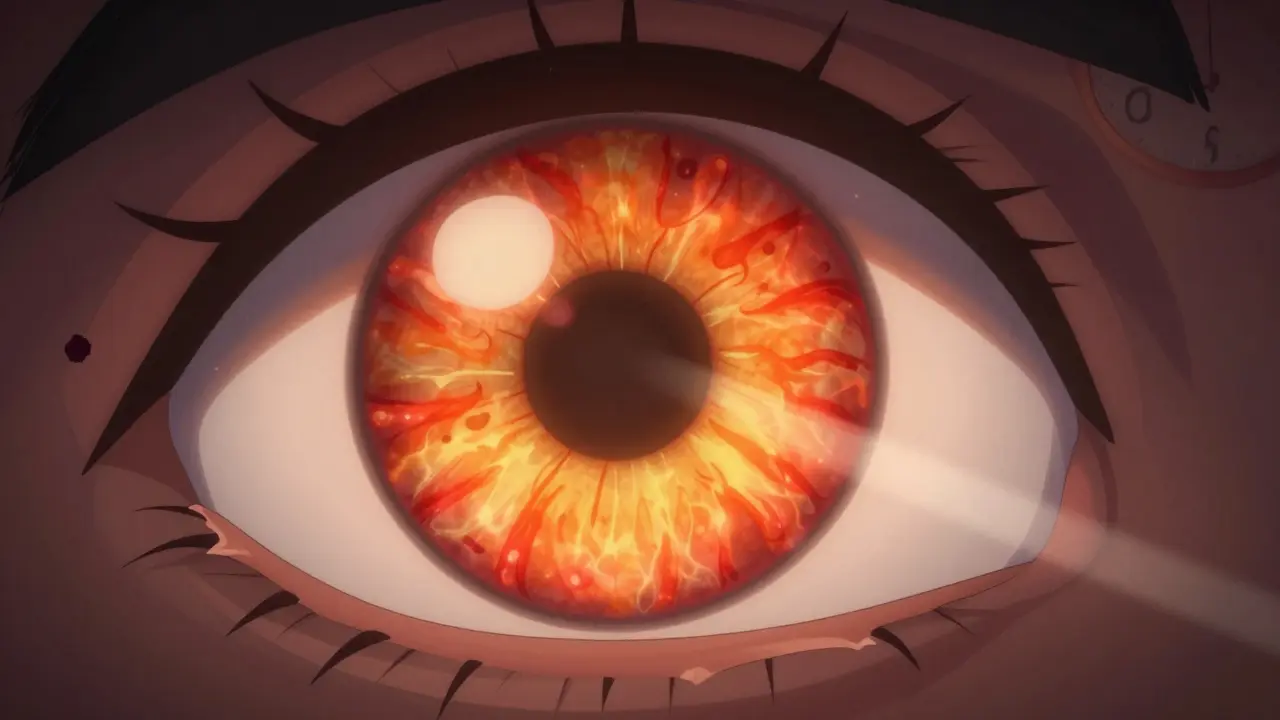
The uvea is the middle layer of your eye, and it’s made up of three parts: the iris (the colored part), the ciliary body (which helps focus your lens), and the choroid (a layer packed with blood vessels that feeds the retina). When any of these parts become inflamed, that’s uveitis. It doesn’t always hurt - sometimes it creeps up silently - but when it does, the damage can be permanent.
There are four main types of uveitis, based on where the inflammation hits:
- Anterior uveitis - This is the most common type, making up 75% to 90% of all cases. It affects the front of the eye - the iris and ciliary body. Symptoms hit hard and fast: redness, sharp pain (especially when reading), light sensitivity, and blurry vision. It often shows up in one eye.
- Intermediate uveitis - Also called pars planitis, this targets the vitreous, the jelly-like fluid in the center of the eye. It rarely causes pain, but floaters and blurry vision are common. This type often becomes chronic, lasting for months or even years, and can lead to swelling in the macula - the part of the retina that gives you sharp central vision.
- Posterior uveitis - This affects the back of the eye: the retina and choroid. It’s the most dangerous type. Vision loss can happen slowly over weeks or months, and it usually affects both eyes. Often, people don’t notice symptoms until the damage is already done. Many cases are found during routine eye exams.
- Panuveitis - This is when inflammation spreads through all layers of the uvea. It combines symptoms from all the others: pain, floaters, blurred vision, and severe risk of permanent damage.
Uveitis can be acute - lasting less than six weeks - or chronic, lasting longer than that. Acute cases usually come on suddenly, while chronic ones creep up over time. Either way, the longer inflammation goes untreated, the higher the chance of scarring, glaucoma, cataracts, or retinal damage.
What Causes Uveitis?
Here’s the tricky part: in about half of all cases, doctors can’t find a clear cause. These are called idiopathic uveitis cases. But when there is a cause, it usually falls into one of three buckets:
- Autoimmune diseases - Your immune system accidentally attacks your eye. Conditions like ankylosing spondylitis, rheumatoid arthritis, multiple sclerosis, and sarcoidosis are common culprits. If you have one of these, your eye doctor should be monitoring you closely.
- Infections - Viruses like herpes simplex (cold sores), herpes zoster (shingles), and cytomegalovirus (CMV) can trigger uveitis. Bacterial infections like syphilis or toxoplasmosis (from undercooked meat or cat litter) are also known causes. Fungal infections like histoplasmosis - common in certain parts of the U.S. - can show up in the eye years after you’ve been exposed.
- Trauma or surgery - A direct injury to the eye, or even eye surgery, can spark inflammation. This type usually clears up with treatment but still needs prompt attention.
It’s not about being “dirty” or “unhealthy.” Uveitis doesn’t come from poor hygiene. It’s often tied to your body’s internal systems, which is why it’s so important to see an eye specialist - not just your GP. If you have unexplained eye symptoms and you’re over 40, or if you have a history of autoimmune disease, you’re at higher risk.
Steroid Therapy: The First Line of Defense
If you’re diagnosed with uveitis, the first thing your eye doctor will likely prescribe is steroids. Not because they’re a cure-all, but because they’re the most effective at quickly calming inflammation before it destroys your vision.
The type of steroid treatment depends entirely on where the inflammation is:
- For anterior uveitis - Steroid eye drops are the go-to. Usually, prednisolone acetate 1%, dropped in several times a day at first, then slowly tapered over weeks. It works fast - often within a few days - but you must stick to the schedule. Stopping too early can make it come back worse.
- For intermediate uveitis - Eye drops don’t reach far enough. Here, doctors often use injections around the eye (periocular) or oral steroids like prednisone. Some patients get tiny implants that release steroids slowly inside the eye over months.
- For posterior uveitis and panuveitis - These need stronger, deeper treatment. Oral steroids are common, sometimes combined with injections directly into the eye (intravitreal). In chronic cases, doctors may add steroid-sparing drugs like methotrexate or azathioprine to reduce long-term steroid use.
Why not just use steroids forever? Because they come with serious side effects. Long-term oral steroids can cause weight gain, high blood sugar, bone thinning, and mood swings. Eye drops can lead to cataracts or glaucoma - especially if used too long or too often. That’s why treatment isn’t about just throwing steroids at the problem. It’s about using the right dose, for the right time, and then stepping down carefully.
For people with recurring uveitis - especially those with autoimmune conditions - doctors may switch to immunomodulatory therapy (IMT). These drugs, like mycophenolate or adalimumab, help control the immune system without the same side effects as steroids. It’s a slower process, but it’s safer for long-term eye health.
Why Speed Matters
Uveitis doesn’t wait. A 2023 study from the National Eye Institute found that patients who waited more than two weeks before seeking treatment were five times more likely to develop permanent vision loss. That’s not a guess - that’s data.
Think of it like a fire. The sooner you put it out, the less damage it does. If you notice:
- Sudden redness in one eye
- Pain that gets worse when you read or focus
- Floaters that don’t go away
- Blurred vision that doesn’t improve with glasses
- Sensitivity to light that makes you squint indoors
- then you need to see an ophthalmologist within 24 hours. Not tomorrow. Not next week. Today.
Many people delay because they think it’s conjunctivitis or allergies. But conjunctivitis doesn’t cause pain when reading. Allergies don’t cause floaters that last for days. If your symptoms are unusual, intense, or persistent - get checked.
What Happens If It’s Not Treated?
Untreated uveitis doesn’t just cause blurry vision. It causes permanent damage:
- Macular edema - Fluid builds up in the macula, the part of your retina that lets you read, drive, and recognize faces. This can cause irreversible blurring.
- Synechiae - The iris sticks to the lens or retina. This blocks normal fluid flow, raises eye pressure, and can lead to glaucoma.
- Cataracts - Chronic inflammation speeds up clouding of the lens. Even with surgery, vision may not fully recover.
- Retinal detachment - In posterior uveitis, inflammation can tear the retina from the back of the eye.
- Optic nerve damage - If the inflammation spreads, it can attack the nerve that sends visual signals to your brain.
One patient from Birmingham, treated in late 2025, had posterior uveitis for eight months before diagnosis. She lost 40% of her central vision. She’s now on long-term immunotherapy and uses a magnifier to read. She says, “I thought it was just tired eyes. I wish I’d gone sooner.”

When to See a Specialist
If you have any of the symptoms above - especially if you’re over 30, have an autoimmune disease, or have had uveitis before - don’t wait. Go to an eye specialist. General eye exams won’t always catch it. You need a dilated exam, often with imaging like OCT (optical coherence tomography) to see swelling in the retina.
Don’t rely on over-the-counter eye drops. They might make the redness go away, but they won’t touch the inflammation underneath. In fact, they might make things worse by masking symptoms.
And if your uveitis comes back? That’s not normal. Recurrent uveitis means there’s likely an underlying condition - and it needs to be found.
Living With Uveitis
Many people with uveitis go into remission with treatment and live normal lives. But it’s not always a one-and-done fix. Some need years of monitoring. Others need lifelong low-dose medication. The goal isn’t just to clear the inflammation - it’s to protect your vision for decades.
Keep your eye doctor informed if you:
- Start new medications (some drugs can trigger uveitis)
- Develop new symptoms like headaches or joint pain
- Notice changes in vision - even small ones
Regular checkups - even when you feel fine - are part of the treatment. Uveitis can hide quietly, waiting to strike again.
Can uveitis go away on its own?
Sometimes, especially in mild anterior cases, inflammation can fade without treatment. But that doesn’t mean it’s safe. Even if symptoms disappear, the damage may still be happening inside the eye. Without proper treatment, the risk of permanent vision loss increases dramatically. Always see an eye specialist - don’t wait to see if it "goes away."
Are steroid eye drops dangerous?
When used correctly under medical supervision, steroid eye drops are safe and life-saving. The danger comes from using them too long, too often, or without monitoring. Long-term use can cause cataracts or glaucoma, which is why doctors carefully taper the dose and check eye pressure regularly. Never self-prescribe or extend use beyond what your doctor recommends.
Can uveitis affect both eyes?
Yes. While anterior uveitis often starts in one eye, intermediate, posterior, and panuveitis frequently affect both. If you’ve had uveitis in one eye, the other eye is at higher risk. That’s why doctors monitor both eyes closely - even if one looks fine.
Is uveitis contagious?
No. Uveitis itself is not contagious. But if it’s caused by an infection like herpes or syphilis, those infections can be passed to others. The eye inflammation, however, is your body’s internal reaction - not something you can catch from someone else.
What’s the difference between uveitis and conjunctivitis?
Conjunctivitis affects the surface of the eye - the white part and inner eyelids. It usually causes redness, itching, and discharge, but little to no pain or light sensitivity. Uveitis affects the inside of the eye and causes deep pain, blurred vision, and sensitivity to light. It’s not just "worse pink eye" - it’s a completely different condition that needs different treatment.
Can children get uveitis?
Yes. Juvenile idiopathic arthritis (JIA) is one of the most common causes of uveitis in children. Kids often don’t complain of symptoms, so routine eye screenings are critical for children with JIA. Early detection can prevent lifelong vision loss.
If you’ve ever wondered why your eye doctor asks so many questions about your health history - now you know. Uveitis isn’t just an eye problem. It’s a signal. And your eyes are telling you something important. Listen. Act. Protect your vision.



One comment
I thought my red eye was just allergies... until I couldn't read my phone without crying. 🥲 Turns out it was anterior uveitis. Steroid drops saved my vision, but man, the side effects? Dry mouth, insomnia, and feeling like a zombie. Still worth it. Don't wait like I did.
This post reads like a TED Talk written by a traumatized ophthalmologist. 🤔 Uveitis isn't just an eye thing - it's your body screaming, 'I'm not okay!' and most people just pop in some Visine and call it a day. We treat symptoms like customer service tickets. But the eye? It's not a widget. It's a cathedral of light and memory. Let it burn, and you lose more than sight - you lose the texture of your own life.
Excellent breakdown. I'm an optometrist in Delhi and see at least 2-3 uveitis cases per week. Many patients delay because they associate red eyes with conjunctivitis. The key differentiator is photophobia + pain on accommodation. Also, in India, toxoplasmosis and tuberculosis are far more common triggers than in the West. Always test for latent TB before starting steroids.
The clinical precision of this exposition is commendable. One must underscore the epistemological necessity of differential diagnosis: uveitis is not a diagnosis, but a syndrome. Its etiological heterogeneity demands a systems-based approach. The overreliance on glucocorticoids, while empirically efficacious, constitutes a therapeutic myopia that obscures the underlying immunopathological architecture. A paradigm shift toward immunomodulatory stewardship is not merely advisable - it is ethically imperative.
Look, I'm not a doctor, but I've had this happen twice. First time, I ignored it for three weeks because I was 'too busy.' Second time? I went in the same day. Big difference. The first time, I got a cataract. Second time, they caught it before the swelling hit my macula. I'm not saying this to scare you - I'm saying this because I wish someone had told me this in plain English before I ruined my vision. It's not 'tired eyes.' It's your body's emergency flare. Don't be the guy who says 'I'll check it tomorrow.' Tomorrow is too late.
As someone who's lived with autoimmune uveitis for 8 years, I want to say: you're not alone. The fear when your vision blurs? The isolation? The way people say 'it's just your eyes' like it's nothing? I get it. But here's the thing - with the right team, you can live a full life. I paint, I hike, I travel. I just need regular checkups and a good eye doctor who listens. If you're reading this and you're scared? You're okay. You're going to be okay.
So let me get this straight. You're telling me I should drop everything and rush to an eye doctor because my eye is red? Like, what am I supposed to do, cancel my Netflix binge? Nah. I'll just squint harder. If my vision goes, at least I'll have had 12 more episodes of that show. Honestly, this post feels like a PSA from a very anxious optometrist who's never seen a good movie.
I love how this post doesn't just dump facts - it gives you a roadmap. But here's what nobody says: uveitis doesn't care if you're rich, healthy, or young. I was 28, vegan, ran marathons. Then one morning, my left eye looked like a tomato. Turns out, my immune system had a grudge. The steroid drops worked, but the anxiety? That stuck. If you're reading this and you've got symptoms? Go. Now. And bring someone with you. Because when your vision starts fading, you forget how to ask for help.
Dude. I had uveitis after a car accident. They put me on prednisone and I gained 20 lbs in 3 weeks. Felt like a balloon. But here's the kicker - I could see again. So yeah, steroids suck. But not seeing your kid's face? That sucks more. I'm on my third flare and now I take my meds like clockwork. No more 'I'll skip today.' I'm alive because I listened. Don't be dumb. Go to the doc.
I think the government is using uveitis to track people. Why else would they push steroids so hard? I read online that eye inflammation is linked to 5G. And what about the implants? Tiny chips? I know a guy who got one and now his dreams are controlled. Don't trust the eye doctors. They're paid by Big Pharma. Get a second opinion. Or a third. Or five. And don't let them touch your eye.
My niece had uveitis at age 6 because of juvenile arthritis. No symptoms. No pain. Just blurry vision. Routine eye exam caught it. Now she's 14, sees fine, plays soccer. If you have autoimmune stuff - even if it's 'just' RA or lupus - get your kid's eyes checked. Every year. No excuses. It's not about fear. It's about love.
I read this entire thing. And I'm just... wow. You really think people are this naive? You really think they don't know that 'red eye' isn't just allergies? I mean, we live in 2025. We have Google. We have TikTok. We have 17 different eye drop brands. And yet? People still wait. I don't get it. I don't get any of it. You don't need a PhD to know: if your eye hurts when you read, you don't have pink eye. You have a problem. Go. Now. Stop scrolling.
In India, toxoplasmosis and TB are major causes. Many patients come late. Steroids help but we need better access to IMT. Also, children with JIA often go undiagnosed. Screening programs work. Need more funding. Simple. No drama. Just action.